Share your science:

Do strict alcohol policies really work?
SHARE YOUR SCIENCE: A recent study shows how alcohol control measures have affected rates of alcohol-related diseases in the Nordic countries over the past 30 years.

Published
Stricter alcohol policies are linked to lower rates of alcohol-attributed diseases. However, our study shows that socio-cultural factors and the strength of enforcement significantly shape the effectiveness of these policies.
Governments in the Nordic countries employ several strategies: high excise taxes, monopolies to control availability, advertising restrictions, drunk driving limits, and age limits. Despite these efforts, cross-border alcohol trade, cultural drinking norms, and changing economic conditions continue to complicate policy effectiveness.
Countries with stricter policies, such as Norway and Sweden, experienced over 20 per cent reductions in diseases such as liver cirrhosis, cardiovascular diseases, certain cancers, and alcohol-induced pancreatitis
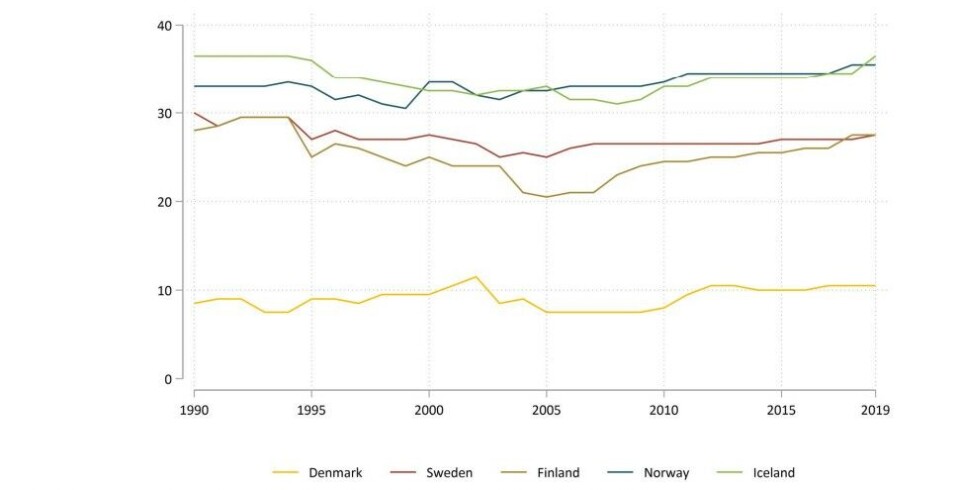
We investigated the effects of alcohol control measures on health outcomes in Denmark, Finland, Iceland, Norway, and Sweden over a 30-year period (1990–2019).
Norway and Iceland stood out with the most restrictive policies, while Denmark maintained minimal controls, resulting in more alcohol-related diseases.
Norway: Strict policies, significant health gains
Norway has one of the most comprehensive alcohol control frameworks in the Nordic region. Vinmonopolet govern when and where alcohol can be sold. Norway’s high distribution control dropped from 1996 due to changes in on-premise sales restrictions.
Key policies include:
- Excise taxes: Norway has among the highest alcohol taxes in the region.
- Legal age limits: A minimum drinking age of 20 for spirits and 18 for beer and wine.
- Advertising ban: Since the 1990s, a strict national ban on alcohol advertising has been enforced.
- BAC (blood alcohol content) limit: Until 2000, Norway’s BAC limit for drivers was 0.05 per cent. This was lowered to 0.02 per cent in 2001.
These policies cut alcohol-related health burdens by over 20 per cent between 1990 and 2019, mainly by reducing chronic conditions like liver cirrhosis. Cross-border alcohol shopping remains a challenge.
Sweden: Balancing policy and control
Sweden controls availability through Systembolaget. Sweden’s complete ban on alcohol advertising was partially lifted in 2004.
Other key policies include:
- BAC limit: Sweden maintains a stringent 0.02 per cent BAC limit.
- Moderate excise taxes: Taxation rates have fluctuated over time.
- Legal age limits: A minimum age of 20 for spirits and 18 for other alcoholic beverages.
Sweden has maintained a relatively high level of restrictiveness over these 30 years. Nevertheless, cultural drinking practices and cross-border trade pose challenges to the effectiveness of Sweden’s alcohol policies.
Iceland: Tough restrictions, mixed results
Iceland enforces some of the strictest alcohol control measures through ÁTVR, its state-run alcohol and tobacco monopoly. The country has permanent restrictions on sales hours, days, and sales locations.
Key policies include:
- High excise taxes: Iceland’s alcohol taxation remains among the highest in the region.
- Marketing restrictions: A full ban on alcohol advertising.
- BAC limit: By 2019, Iceland reduced its BAC limit to 0.02 per cent.
- Legal age limits: Iceland enforces a 20-year minimum drinking age for spirits and 18 for other beverages.
Despite these strict rules, alcohol-related health issues in Iceland rose by 14 per cent from 1990 to 2019. Researchers link this to changing economy and drinking habits.
Denmark: Minimal controls, high disease burden
Denmark adopts a lenient approach to alcohol control. The country lacks a state monopoly on alcohol production and distribution, and sales regulations are limited.
Key policies include:
- Gradual introduction of age limits: Modest improvements followed the introduction of age limits for off-premise sales in 2012, requiring consumers to be at least 18 to purchase certain alcoholic beverages.
- Relaxed marketing rules: Advertising is governed by statutory control rather than a complete ban, limiting the impact of marketing restrictions on youth exposure.
- Higher BAC limit: Denmark’s BAC limit of 0.05 per cent is more lenient than in other Nordic countries, contributing to greater alcohol tolerance among drivers.
Men responded more to alcohol price hikes and restrictions. Women faced more mental health risks from alcohol, while men had higher dependence.
These policy weaknesses have contributed to Denmark’s high alcohol-attributed disease burden. Low enforcement and limited deterrent measures hinder efforts to control alcohol-related harm.
Finland: Policies in flux
Finland’s alcohol policies have fluctuated over time. Initially, strict state control defined Finland’s approach, but EU membership in the mid-1990s led to liberalisation, replacing many off-premise sales restrictions with a licensing system and resulting in inconsistent excise taxes.
Key policies include:
- Loosened state monopoly: Shifting to a licensing system weakened distribution control.
- Eased marketing restrictions: Finland transitioned from a full advertising ban to statutory control, reducing efforts to limit youth exposure to alcohol.
- Binge drinking culture: Strong social drinking traditions, including binge drinking, have counteracted policy effectiveness.
- Cross-border trade: Lower alcohol prices in neighbouring countries have led to increased cross-border alcohol purchases, undermining local control efforts.
Despite these challenges, Finland maintains low BAC limits and prevention programs to mitigate alcohol-related risks. However, fluctuating policies and external factors have limited the success of these measures.
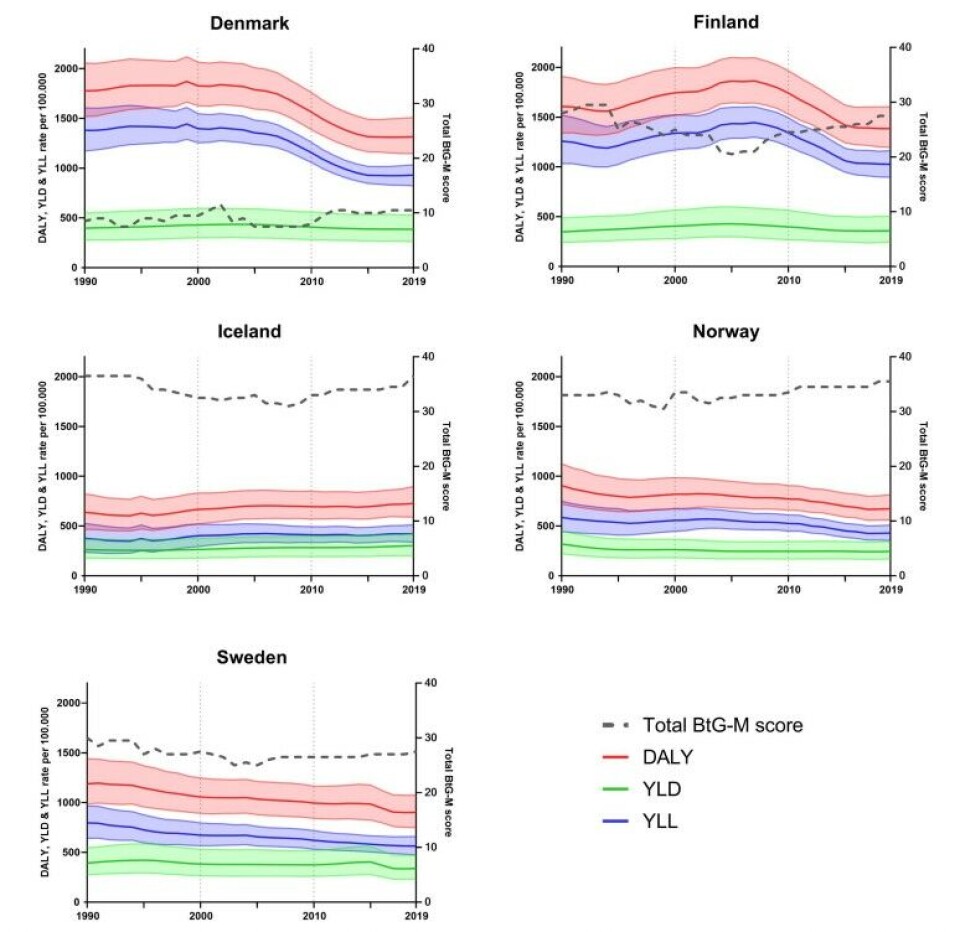
Health outcomes and policy challenges
From 1990 to 2019, alcohol-related health issues dropped in all Nordic countries except Iceland. Countries with stricter policies, such as Norway and Sweden, experienced over 20 per cent reductions in diseases such as liver cirrhosis, cardiovascular diseases, certain cancers, and alcohol-induced pancreatitis.
Immediate causes such as alcohol poisoning, traffic injuries, self-harm, and violence-related injuries showed mixed but notable improvements, particularly in younger male populations.
Men responded more to alcohol price hikes and restrictions. Women faced more mental health risks from alcohol, while men had higher dependence.
The reductions highlight the importance of comprehensive, well-enforced alcohol policies that address both delayed and immediate health risks. Future public health campaigns aimed at raising awareness of alcohol's harmful effects—especially those targeting younger at-risk groups—could complement these regulatory measures to further sustain and enhance the gains in reducing alcohol-related harm.
References:
- van der Velde L, Shabaan AN, Månsson A, Wennberg P, Allebeck P, Karlsson TG, Flodin P, Eikemo TA, Skrindo Knudsen AK, de Soysa I, Skogen JC; GBD 2019 Nordic Alcohol Collaborators; Gissler M, McGrath JJ, Sigfusdottir ID, Sigurvinsdottir R, Pasovic M, Danielsson AK, Agardh EE. Alcohol-attributed disease burden and formal alcohol policies in the Nordic countries (1990-2019): an analysis using the Global Burden of Disease Study 2019. Eur J Public Health. 2024 Dec 2:ckae195. doi: 10.1093/eurpub/ckae195. https://academic.oup.com/eurpub/advance-article/doi/10.1093/eurpub/ckae195/7915047?login=true
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020 Oct 17;396(10258):1204-1222. doi: 10.1016/S0140-6736(20)30925-9. https://www.sciencedirect.com/science/article/pii/S0140673620309259?via%3Dihub
Further reading:


Share your science or have an opinion in the Researchers' zone
The ScienceNorway Researchers' zone consists of opinions, blogs and popular science pieces written by researchers and scientists from or based in Norway.
Want to contribute? Send us an email!




















